Potential Gaps in Data Submission |
Back to Common Failures Back to HCC Risk Adjustment |
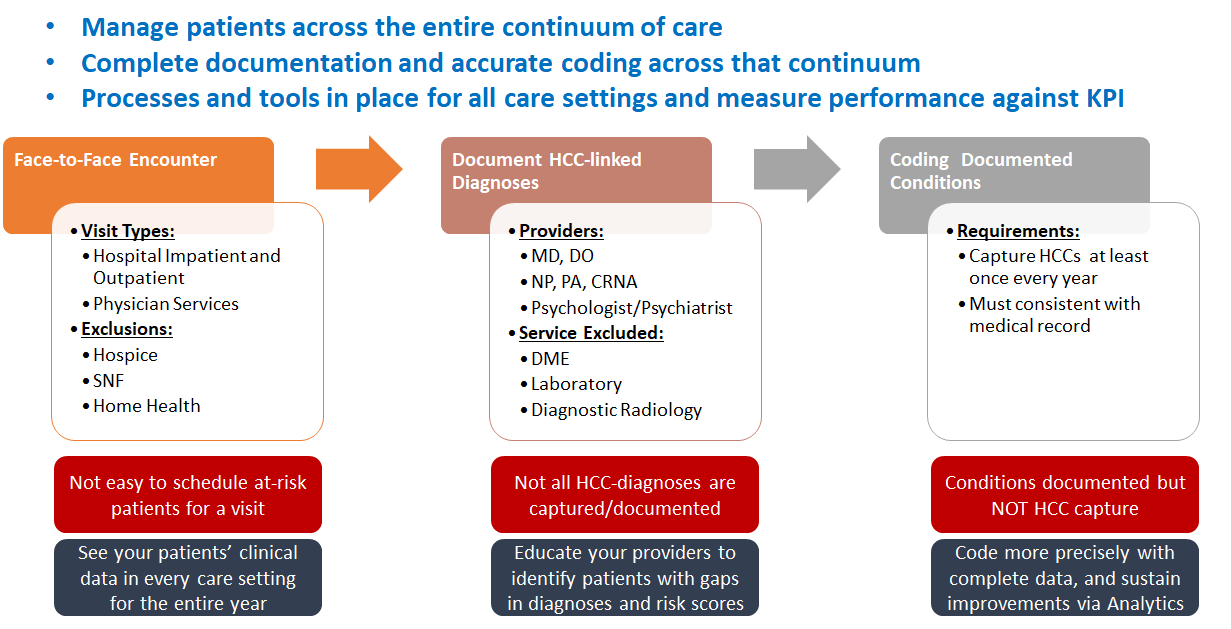
To accurately report the severity of a member’s illness that affects care and treatment and to comply with the Centers for Medicare and Medicaid Services for a valid HCC, a provider must document in the medical record the clinical findings with supportive details:
- See Each Patient at Least Once Each Year
The health status of a Medicare Advantage patient needs to be redetermined each year. Diagnoses from a prior year do not “carry over” for CMS.
- Evaluate and Document All Chronic Conditions
All conditions that constitute the “composite health picture” of the senior patient should be evaluated and documented clearly and legibly in the progress note of the medical record. This is not limited to what brought the patient to the doctor today. What other conditions is the patient dealing with every day?
- Code All Diagnoses
The coder must be careful to capture all diagnoses that have been properly documented. Does the coder have access to the latest ICD-10-CM codes? Does the coder code to the highest level of specificity to accurately report the level of disease severity?
- Accurate coding affects provider payments and settlement outcomes. Use an Accurate, Up-to-date Superbill (or Favorites List in EMR)
If a superbill is used, does it contain a wide variety of ICD-10-CM codes to allow the specificity of the disease to be coded accurately? Is it up to date? Are providers trained to write in additional diagnoses if they apply or do they use the closest match on the superbill instead? Is the superbill evaluated each year to ensure it meets the needs of the practice?
- Make Sure the Data is Captured
The provider must be aware of the limitations of their practice management system. How many diagnosis codes does the system allow? Is there potential for any codes to be dropped? Is the provider correctly sequencing the diagnoses?
- The Claim or Encounter Format or Form Must Contain All the Data
When the data is extracted for claims or encounter reporting, are all diagnosis codes extracted to be sent to the health plan? Does the claim process limit the number of diagnoses that can be submitted? Is the practice in the habit of only sending one or two diagnosis codes to support the CPT code on the claim?
- Verify that Clearinghouse or Submission Vendor Can Send and Receive All Recorded Codes
How many codes can the vendor support for data submission? Are valid codes being dropped because the provider has not updated the number of codes that can be submitted? Many claims systems and practice management systems are being enhanced to capture more data due to HIPAA data requirements. Has the vendor’s submission been expanded to accept additional data as well?
- Verify that Health Plans Can Send and Receive All Recorded Codes
Not all health plans have expanded their systems to accept large numbers of diagnosis codes. How many codes can your payer accept? What happens to any codes submitted beyond the accepted number? Is there an alternative submission method (ASM) available?